

In the present study, we explored the anticancer effect of cannabidiol loaded magnesium-gallate (CBD/Mg-GA) metal-organic framework (MOF) using the rat glioma brain cancer (C6) cell line.
Bioactive and microporous magnesium gallate MOF was employed for simultaneous delivery of two potential anticancer agents (gallic acid and CBD) to the cancer cells. Gallic acid (GA), a polyphenolic compound, is part of the MOF framework, while CBD is loaded within the framework. Slow degradation of CBD/Mg-GA MOF in physiological fluids leads to sustained release of GA and CBD.
CBD’s anti-cancer actions target mitochondria, inducing their dysfunction and generation of harmful reactive oxygen species (ROS). Anticancer effects of CBD/Mg-GA include a significant increase in ROS production and a reduction in anti-inflammatory responses as reflected by a significant decrease in TNF-α expression levels. Molecular mechanisms that underlie these effects include the modulation of NF-κB expression, triggering the apoptotic cascades of glioma cells. CBD/Mg-GA MOF has potential anti-cancer, anti-inflammatory and anti-oxidant properties.
Thus, the present study demonstrates that CBD/Mg-GA MOF may be a promising therapeutic for glioblastoma.”
https://pubmed.ncbi.nlm.nih.gov/33657198/
https://pubs.rsc.org/en/content/articlelanding/2021/TB/D0TB02780D#!divAbstract
 “Preclinical data suggest some cannabinoids may exert antitumour effects against glioblastoma (GBM). Safety and preliminary efficacy of nabiximols oromucosal cannabinoid spray plus dose-intense temozolomide (DIT) was evaluated in patients with first recurrence of GBM.
“Preclinical data suggest some cannabinoids may exert antitumour effects against glioblastoma (GBM). Safety and preliminary efficacy of nabiximols oromucosal cannabinoid spray plus dose-intense temozolomide (DIT) was evaluated in patients with first recurrence of GBM.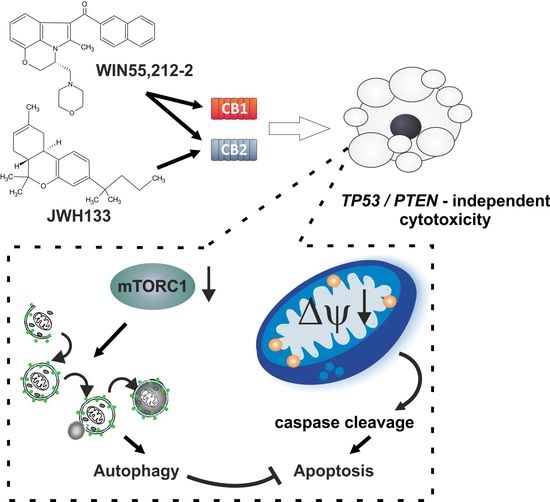
 “Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant.
“Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant. “Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”
“Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”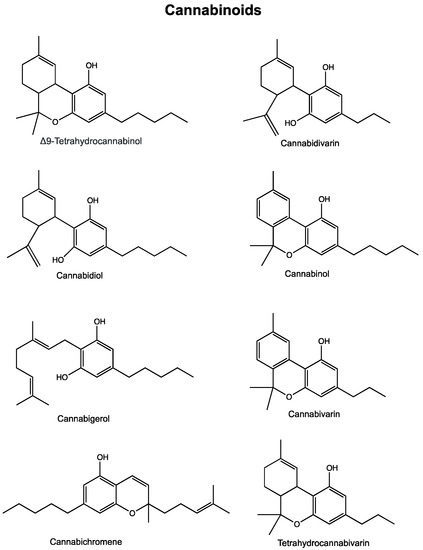
 “Astrocytomas, the most prevalent primary brain tumors, can be divided by histology and malignancy levels into four following types: pilocytic astrocytoma (grade I), diffuse fibrillary astrocytoma (grade II), anaplastic astrocytoma (grade III), and glioblastoma multiforme (grade IV). For high grade astrocytomas (grade III and grade IV), blood vessels formation is considered as the most important property.
“Astrocytomas, the most prevalent primary brain tumors, can be divided by histology and malignancy levels into four following types: pilocytic astrocytoma (grade I), diffuse fibrillary astrocytoma (grade II), anaplastic astrocytoma (grade III), and glioblastoma multiforme (grade IV). For high grade astrocytomas (grade III and grade IV), blood vessels formation is considered as the most important property.