

“Endocannabinoids are host-derived lipid hormones that fundamentally impact gastrointestinal (GI) biology. The use of cannabis and other exocannabinoids as anecdotal treatments for various GI disorders inspired the search for mechanisms by which these compounds mediate their effects, which led to the discovery of the mammalian endocannabinoid system. Dysregulated endocannabinoid signaling was linked to inflammation and the gut microbiota. However, the effects of endocannabinoids on host susceptibility to infection has not been explored. Here, we show that mice with elevated levels of the endocannabinoid 2-arachidonoyl glycerol (2-AG) are protected from enteric infection by Enterobacteriaceae pathogens. 2-AG directly modulates pathogen function by inhibiting virulence programs essential for successful infection. Furthermore, 2-AG antagonizes the bacterial receptor QseC, a histidine kinase encoded within the core Enterobacteriaceae genome that promotes the activation of pathogen-associated type three secretion systems. Taken together, our findings establish that endocannabinoids are directly sensed by bacteria and can modulate bacterial function.”

 “Cannabis has been used for its medicinal purposes since ancient times. Its consumption leads to the activation of Cannabis receptors CB1 and CB2 that, through specific mechanisms can lead to modulation and progression of inflammation or repair. The novel findings are linked to the medical use of Cannabis in gastrointestinal (GI) system.
“Cannabis has been used for its medicinal purposes since ancient times. Its consumption leads to the activation of Cannabis receptors CB1 and CB2 that, through specific mechanisms can lead to modulation and progression of inflammation or repair. The novel findings are linked to the medical use of Cannabis in gastrointestinal (GI) system. “The cannabis plant has been widely researched for many therapeutic indications and found to be effective in many chronic conditions such as epilepsy, neuropathic or chronic pain and more. However, biased opinion against compounds of the plant, regulatory as well as compounding challenges have led to very few approved medicinal products. Those formulations which are approved are dosed several times a day, creating an unmet need for controlled release (CR) formulations of
“The cannabis plant has been widely researched for many therapeutic indications and found to be effective in many chronic conditions such as epilepsy, neuropathic or chronic pain and more. However, biased opinion against compounds of the plant, regulatory as well as compounding challenges have led to very few approved medicinal products. Those formulations which are approved are dosed several times a day, creating an unmet need for controlled release (CR) formulations of 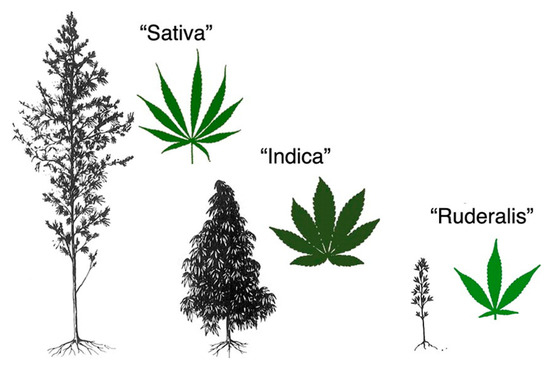
 “Many anti-nausea treatments are available for chronic gastrointestinal syndromes, but data on efficacy and comparative effectiveness are sparse.
“Many anti-nausea treatments are available for chronic gastrointestinal syndromes, but data on efficacy and comparative effectiveness are sparse. “Chronic intestinal pseudo-obstruction (CIPO) is a rare and challenging cause of pediatric intestinal failure, requiring long-term parenteral nutrition in most cases. Despite optimal management, some patients experience chronic abdominal pain and recurrent obstructive episodes with a major impact on their quality of life.
“Chronic intestinal pseudo-obstruction (CIPO) is a rare and challenging cause of pediatric intestinal failure, requiring long-term parenteral nutrition in most cases. Despite optimal management, some patients experience chronic abdominal pain and recurrent obstructive episodes with a major impact on their quality of life. “A growing body of literature indicates that activation of
“A growing body of literature indicates that activation of  “Irritable bowel syndrome (IBS) global burden is underestimated despite its high prevalence. It’s a gastrointestinal disease having obscure pathophysiology with multiple therapies yet unsatisfactory remedies.
“Irritable bowel syndrome (IBS) global burden is underestimated despite its high prevalence. It’s a gastrointestinal disease having obscure pathophysiology with multiple therapies yet unsatisfactory remedies. “Irritable bowel syndrome (IBS) is one of the most common functional gastrointestinal (GI) disorders characterized by pain and impaired bowel movements. Currently available drugs show limited efficacy.
“Irritable bowel syndrome (IBS) is one of the most common functional gastrointestinal (GI) disorders characterized by pain and impaired bowel movements. Currently available drugs show limited efficacy.