“Pulmonary hypertension (PH) is a severe and incurable disease that may lead to right ventricular (RV) failure and consequently, death. The remodeling of small pulmonary vessels, perivascular lung tissue and RV plays a key role in the PH development.
Cannabidiol (CBD) is a non-intoxicating compound of Cannabis and has a multidirectional beneficial properties, including antiproliferative.
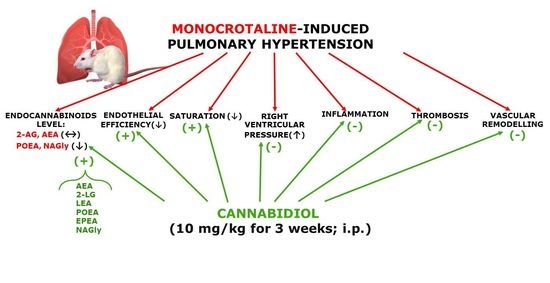
The aim of the study was to investigate if CBD possess the antifibrotic potential in the lung and RV of rats with monocrotaline (MCT)-induced PH.
The studies were carried out on rats with (MCT; 60 mg/kg, subcutaneously (s.c.)) and without PH (control group). CBD (10 mg/kg) or its vehicle were administered once daily, intraperitoneally (i.p.), for 3 weeks after administration of MCT or its vehicle. Western blot and immunohistochemistry methods were used.
In the lung and RV of the rats with MCT-induced PH, an increase of galectin-3, the growth transforming factor beta 1 (TGF-β1), collagen I expression and a greater number of mast cells, which are the cells responsible for lung remodeling were observed. CBD reduced the expression of above-mentioned profibrotic parameters and the number of mast cells in the lungs and/or RV of rats with MCT-induced PH.
In conclusion, CBD has potential property to inhibit lung and RV remodeling, possibly by inhibiting the TGF-β1-dependent pathway and may be considered as an adjuvant therapy in the treatment of PH.”