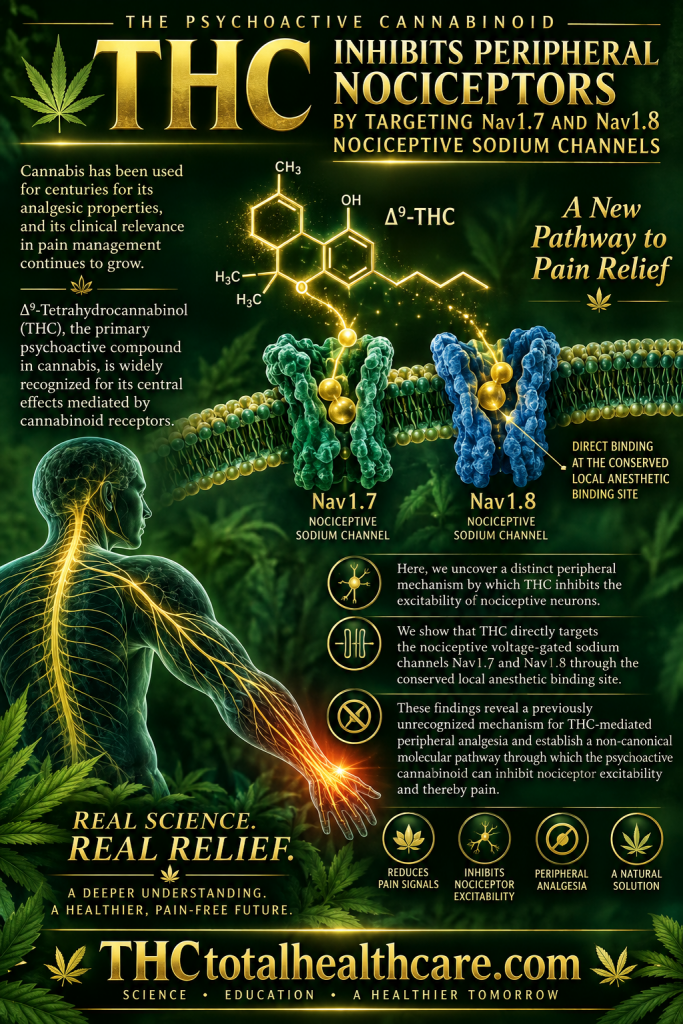
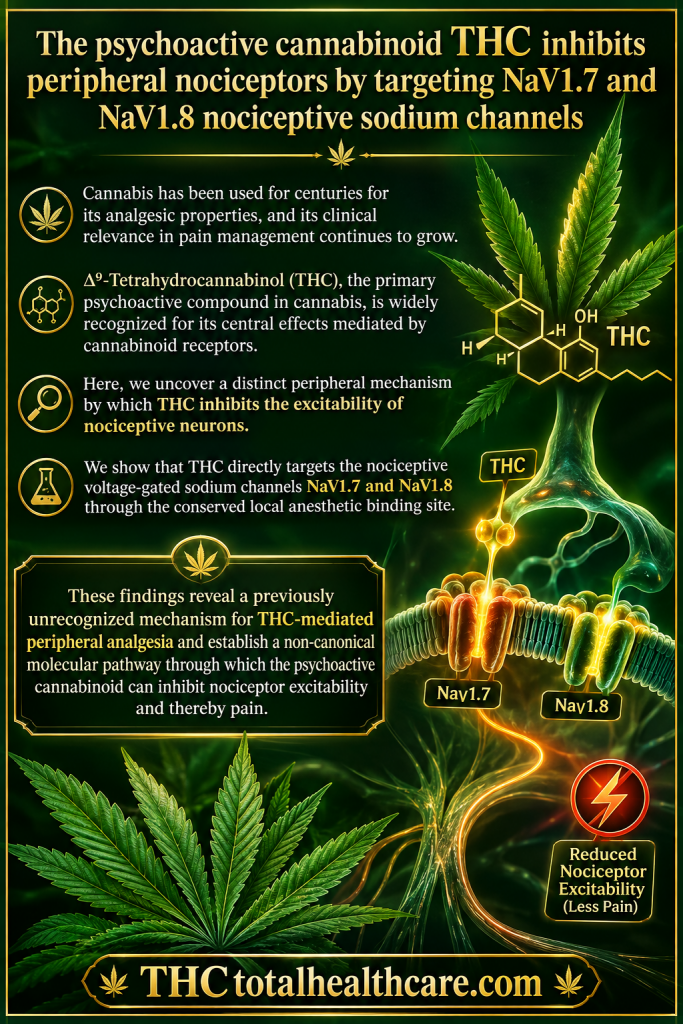
“Δ⁹-Tetrahydrocannabinol (THC), the primary psychoactive compound in cannabis, is widely recognized for its central effects mediated by cannabinoid receptors. Here, we uncover a distinct peripheral mechanism by which THC inhibits the excitability of nociceptive neurons.
We show that THC directly targets the nociceptive voltage-gated sodium channels NaV1.7 and NaV1.8 through the conserved local anesthetic binding site. This interaction reduces sodium currents and suppresses action potential generation in peripheral sensory neurons.
Our findings demonstrate that, beyond its central psychoactivity, THC exerts direct peripheral nociceptor inhibition via modulation of NaV1.7 and NaV1.8, offering new insight into cannabinoid-based analgesia independent of cannabinoid receptor signaling.”
“Cannabis has been used for centuries for its analgesic properties, and its clinical relevance in pain management continues to grow.”
“These findings reveal a previously unrecognized mechanism for THC-mediated peripheral analgesia and establish a non-canonical molecular pathway through which the psychoactive cannabinoid can inhibit nociceptor excitability and thereby pain.”
“Background: Ischemic stroke is an acute neurological disorder with limited treatment options. Medical cannabinoids (MCs), primary bioactive compounds extracted from cannabis plants, have shown therapeutic prospects for ischemic stroke. This study integrates bibliometrics and meta-analysis to comprehensively summarize the research landscape of MCs in cerebral ischemia and thoroughly investigate their role and potential mechanisms in ischemic stroke.
Methods: Bibliometric analysis was performed based on literature retrieved from Web of Science Core Collection (WoSCC), PubMed, and Scopus. For meta-analysis, a comprehensive search was conducted across four databases (WoSCC, PubMed, Embase, and Cochrane Library) and grey literature repositories. Studies were screened according to predefined criteria. Pooled standardized mean differences with 95% confidence interval were calculated, followed by subgroup analysis.
Results: A total of 241 publications were identified for bibliometric analysis. From 2000 to June 2025, the annual publication output on MCs in cerebral ischemia displayed a fluctuating yet overall upward trend. Keyword co-occurrence analysis revealed three major research topics: neuroprotective mechanisms of MCs, pathological models of cerebral ischemia, and bioactive components of MCs. Meta-analysis of 26 studies demonstrated that MCs provided significant neuroprotection in animal models of ischemic stroke, including cerebral infarct volume, neurological function score (NFS), cerebral blood flow (CBF), blood-brain barrier (BBB) permeability, brain water content, apoptosis (TUNEL-positive cells), oxidative stress markers, inflammation (TNF-α, IL-1β), and excitotoxicity (Glu/NAA, Lac/NAA ratio). Subgroup analysis revealed that intraperitoneal administration and a full-course of cannabidiol (CBD) treatment were associated with reduced heterogeneity and enhanced therapeutic benefit. Isoflurane was identified as a potentially suitable anesthetic.
Conclusion: MCs exert multi-target neuroprotection in ischemic stroke by improving CBF, reducing brain edema and BBB permeability, and inhibiting oxidative stress, neuroinflammation, apoptosis, and excitotoxicity. Future research should focus on high-quality clinical trials to validate these findings and translate MCs into clinical practice.”
“CBD acts as a negative allosteric modulator of cannabinoid receptors (CBR) and exerts brain-protective effects through multi-target regulatory properties “
“Moreover, the results of meta-analysis consolidate preclinical evidence, demonstrating that MCs confer neuroprotection by mitigating multiple pathological processes, including cerebral tissue perfusion, BBB permeability and cerebral edema, oxidative stress, excitotoxicity, inflammatory responses, and apoptosis.”
“Chronic musculoskeletal pain (CMP) is a pervasive condition that can impair daily functioning and quality of life. Traditional pharmaceutical therapies, including non-steroidal anti-inflammatory drugs, gabapentinoids, and opioids, often yield suboptimal results and carry notable risks, such as adverse side effects and dependence.
Increasing interest has turned toward medical cannabis, particularly combined formulations of cannabidiol (CBD) and tetrahydrocannabinol (THC), as a potential alternative or complement to current pain management strategies.
Evidence suggests that cannabinoids interact with the endocannabinoid system to modulate nociception and inflammation, offering meaningful pain relief and possibly reducing opioid requirements.
However, heterogeneity in study designs, product formulations, and regulatory frameworks presents challenges in drawing definitive conclusions. Additionally, while most adverse effects, such as fatigue, dizziness, and mild cognitive changes, are generally reported as tolerable, concerns remain about long-term safety and standardization of dosing.
Taken together, the existing literature points to a promising role for medical cannabis in CMP management, underscoring the need for further high-quality research to establish best practices, clarify patient selection, and guide clinicians in safe and effective cannabinoid therapy.”
“This scoping review highlights the potential role of medical cannabis in managing musculoskeletal pain. Evidence suggests it may reduce pain, enhance well-being, and improve quality of life, particularly as an alternative or adjunct to opioids. Adverse effects are typically mild, supporting its use as a safer long-term option. However, data on long-term efficacy, especially for CBD, remain limited.
Given the risks of opioid dependence, cannabis offers a promising therapeutic alternative.”
“Cannabis sativa yields a wide range of bioactive compounds, including terpenes, flavonoids, and cannabinoids.
Tetrahydrocannabinolic acid (THCA), cannabidiolic acid (CBDA), cannabigerolic acid (CBGA), and cannabichromenic acid (CBCA) are the acidic biosynthetic precursors of the neutral cannabinoids Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD), which have been the subject of much research.
This review examines the biosynthesis, decarboxylation, molecular pharmacology, and therapeutic significance of acidic cannabinoids, intending to address a significant knowledge gap. Peer-reviewed literature from major scientific databases was used in a systematic narrative review with an emphasis on investigations of acidic cannabinoid chemistry, pharmacology, pharmacokinetics, and disease-specific applications.
According to the reviewed data, acidic cannabinoids exhibit unique biological activities that distinguish them from their neutral counterparts. These include neuroprotective, anti-inflammatory, anticonvulsant, and anti-proliferative actions, which are mediated by molecular targets such as serotonin 5-HT1A receptors, cyclooxygenase-2 (COX-2), transient receptor potential (TRP) channels, and peroxisome proliferator-activated receptor-γ (PPARγ).
Acidic cannabinoids are more appealing for therapeutic usage in children and the elderly, considering that they are not intoxicating like THC; however, this distinction applies primarily to non‑heated consumption. Chemical instability, low bioavailability, and a dearth of controlled human trials impede clinical translation despite their potential.
According to the findings, acidic cannabinoids are an underutilized yet potentially valuable class of precision medicines.
In this study, we outline existing understanding on acidic cannabinoids, discuss their production and transformation, and identify research needs that could influence cannabis science research.”
“The high metastatic potential of melanoma and its poor prognosis in advanced stages motivate the search for innovative therapeutic approaches. Therefore, this study aimed to assess the effects of phytocannabinoids (cannabidiol-CBD, and cannabigerol-CBG) on the structure and function of the melanoma cell membrane, phospholipid metabolism, and the respective metabolites generated in ROS- and enzyme-dependent reactions.
Biochemical and physicochemical parameters were analyzed in melanoma cells (SK-MEL-5) cultured for 24 h with CBD (5 µM), CBG (1 µM), and their combination applied either alone or after UVA irradiation (365 nm) at a dose of 18 J/cm².
Phytocannabinoids have been shown to partially counteract changes in the levels of cell membrane components, including phospholipid polyunsaturated fatty acids (PUFAs) and sialic acid, consequently affecting surface charge density and lipid rafts, which may be a potential target for anticancer therapy. Furthermore, by changing the activity of lipolytic enzymes (PLA2/COX1/2/LOX-5), phytocannabinoids partially enhanced the UVA-induced decrease in free PUFAs. Consequently, the levels of lipid mediators, including endocannabinoids and eicosanoids, were altered.
The use of phytocannabinoids led to a significant increase in 2-AG levels, while the combined action of CBD/CBG reduced the levels of pro-inflammatory eicosanoids. UVA radiation increased the expression of G-protein-coupled receptors in melanoma cells (CB1/2/TRPV1/PPARγ), while the combined use of CBD/CBG reduced their expression.
Therefore, the results have shown that CBD and CBG modulate the metabolism of phospholipids and PUFAs by altering the functions of melanoma cell membranes, potentially offering options for the use of these phytocannabinoids in the integrative biomedicine treatment of melanoma.”
“In summary, the results of this study indicate that phytocannabinoids (CBD and/or CBG) alter the functionality of melanoma cell membranes by modeling the structure and metabolism of phospholipids and free PUFAs, which may offer potential benefits in integrated melanoma therapy.”
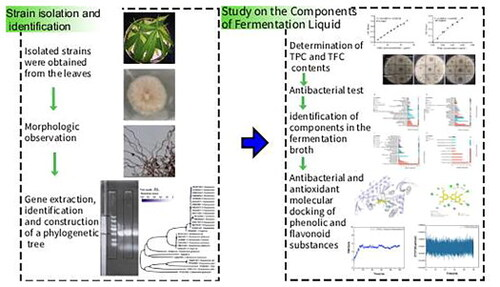
“Endophytic fungi are prolific sources of natural antioxidants and antibacterial agents.
This study aims to isolate and identify the endophytic fungus EFY14 from Cannabis sativa L. leaves and to evaluate the antibacterial and antioxidant activities of its culture filtrates.
Non-targeted metabolomics was employed to chemically profile the EFY14 crude extract, a potential biological targets were predicted through molecular docking and molecular dynamics simulations. EFY14 was taxonomically identified as belonging to the Chaetomium genus.
Its extract contained 20.823 ± 1.449 mg gallic acid equivalent (GAE)/L total phenolic and 0.230 ± 0.007 mg rutin equivalent (RE)/mL total flavonoids, displaying antioxidant and antibacterial activities. Metabolomic profiling identified flavonoids and phenolic compounds, including 4′,7-dihydroxy-8-methylisoflavone, scopoletin, xanthohumol, tricin, sophoraflavanone G, prenyl glucoside, melilotoside and maltol. Molecular docking indicated potential molecular targets for these metabolites.
These findings suggest that EFY14 derived endophytic fungi from C. sativa L. may represent a novel source of antioxidant and antibacterial compounds.”
“In this study, a strain named Chaetomium globusum EFY14 was identified from the leaves of the Cannabis genus plants. It was determined to be a new source of antioxidants and antibacterial agents. Additionally, the Cannabidiolic acid component was detected through metabolomics. The extract is rich in phenolic and flavonoid substances and has DPPH scavenging activity as well as inhibitory activity against E.coli, B.subtilis, and S.aureus. The metabolites verified through metabolomics and molecular docking provide promising candidate substances for drug development and agricultural biological control, as well as new methods for cannabinoid synthesis.”
“This research is highly relevant for professionals in the fields of pharmaceuticals, agriculture and natural products. The identification of Chaetomium globusum. EFY14 from the Cannabis genus as a source of phenolic substances, flavonoids (such as xanthohumol, tricin) and antioxidant/antibacterial metabolites provides feasible development leads for new drugs, biological pesticides and natural antioxidants. This strain offers new strains for industrial production of antioxidant and antibacterial substances.”
“Breast cancer remains a leading cause of cancer-related morbidity and mortality globally, highlighting the urgent need for novel therapeutic strategies.
This study investigates the molecular mechanisms underlying the anti-proliferative potential of Cannabis sativa dichloromethane extract (C. sativa DCM) on oxidative stress, apoptosis, and invasion in human breast cancer cells.
Key biomarkers, such as antioxidant enzymes (Superoxide Dismutase (SOD) and Glutathione (GSH)), the transcription factor Nrf2, apoptotic proteins (p53, caspase-8 and 9), metalloproteinase (MMP-1 and MMP-9), and Transforming Growth Factor Beta (TGF-β) were examined. Cytotoxicity was assessed using an MTT assay in the MDA-MB-231 and MCF-7 breast cancer cell lines, with comparisons to normal skin fibroblasts (HS27). Oxidative stress biomarkers were quantified using enzymatic assays and ELISA kits, while apoptotic and anti-metastatic factors were determined by Western blotting.
Results demonstrated that C. sativa DCM extract induced significant cell death in a concentration-dependent manner, with IC50 values of 75.46 ± 0.132 μg/mL for MDA-MB-231 and 78.68 ± 0.50 μg/mL for MCF-7 cells. The extract decreased SOD and GSH levels while increasing p53 and caspase activity, confirming apoptosis activation. Additionally, C. sativa DCM inhibited migration and invasion by downregulating MMP-1, MMP-9, and TGF-β. The anti-proliferative potential of C. sativa DCM in breast cancer cells is mediated through a continuous biological pathway involving oxidative stress modulation, apoptotic signaling, and anti-invasive effects. Phytochemical analysis revealed terpenoids and steroids, including compounds like cannabidiol and tetrahydrocannabinol acid.
These findings suggest that C. sativa DCM extract holds potential as an anti-breast cancer therapeutic and warrants further preclinical and clinical investigations.”
“Cannabis sativa L., known in many slang languages as marijuana, bhang, ganja, for instance, is an herbaceous species originating from Central Asia and widely distributed around the world. It has been used as a source of fiber, food, oil, and for its multiple curative properties, including anti-parasitic, antipyretic, antibacterial, antitumor, vermifuge, dermatic, and pain-killing properties for centuries. Phytocannabinoids, derived from cannabis, have shown anti-cancer activity in cell lines”
“Based on these research findings, we concluded that C. sativa DCM extract possesses the potential to inhibit the proliferation of breast cancer cells (MCF-7 and MDA-MB-231), while exhibiting minimal cytotoxic effect on normal skin cells Hs27.”
“Given these conclusive findings, the presence of bioactive phytochemicals in C. sativa DCM can be considered as a potential source of anti-cancer agents.”
“Autophagy is a well-preserved biological mechanism that is essential for sustaining homeostasis by degradation and recycling damaged organelles, misfolded proteins, and other cytoplasmic detritus.
Cannabinoid signaling has emerged as a prospective regulator of diverse cellular functions, including immunological modulation, oxidative stress response, apoptosis, and autophagy. Dysregulation of autophagy contributes to pathogenesis and treatment resistance of several oral diseases, including oral squamous cell carcinoma (OSCC), periodontitis, and gingival inflammation.
This review delineates the molecular crosstalk between cannabinoid receptor type I (CB1) and type II (CB2) activation and autophagic pathways across oral tissues. Cannabinoids, including cannabidiol (CBD) and tetrahydrocannabinol (THC), modulate key regulators like mTOR, AMPK, and Beclin-1, thereby influencing autophagic flux, inflammation, and apoptosis.
Experimental studies indicate that cannabinoids inhibit the PI3K/AKT/mTOR pathway, promote reactive oxygen species (ROS)-induced autophagy, and modulate cytokine secretion, mechanisms that underline their dual anti-inflammatory and anti-cancer capabilities. In addition, cannabinoid-induced autophagy has been shown to enhance stem cell survival and differentiation, offering promise for dental pulp regeneration. Despite these promising prospects, several challenges remain, including receptor selectivity, dose-dependent variability, limited oral bioavailability, and ongoing regulatory constraints.
A deeper understanding of the context-dependent regulation of autophagy by cannabinoid signaling could pave the way for innovative therapeutic interventions in dentistry. Tailored cannabinoid-based formulations, engineered for receptor specificity, tissue selectivity, and optimized delivery, hold significant potential to revolutionize oral healthcare by modulating autophagy-related molecular pathways involved in disease resolution and tissue regeneration.”
“Cannabinoids are a diverse class of bioactive lipophilic compounds derived from Cannabis sativa and other plant species, as well as synthesized endogenously and pharmacologically, and have attracted significant attention for their immunomodulatory, anti-inflammatory, antioxidant, and anticancer effects.”
“Cannabinoid-based treatments show promise for managing oral diseases by controlling inflammation and promoting tissue regeneration through specific pathways.”
“Paediatric acute-onset neuropsychiatric syndrome (PANS) is a syndrome of infection-provoked abrupt-onset obsessive-compulsive disorder (OCD) or eating restriction.
Based on the hypothesis that PANS is an epigenetic disorder of immune and brain function, a full-spectrum medicinal cannabinoid-rich low-THC cannabis (NTI164) was selected for its known epigenetic and immunomodulatory properties.
This open-label trial of 14 children with chronic-relapsing PANS (mean age 12·1 years; range 4-17; 71 % male) investigated the safety and efficacy of 20 mg/kg/day NTI164 over 12 weeks. Clinical outcomes were assessed using gold standard tools. To define the biological effects of NTI164, blood samples were collected pre- and post-treatment for bulk and single-cell transcriptomics, proteomics, phosphoproteomics, and DNA methylation.
NTI164 was well-tolerated, and 12 weeks of treatment decreased the mean Clinical Global Impression-Severity (CGI-S) score from 4·8 to 3·3 (p = 0·002). Significant improvements were observed in emotional regulation (RCADS-P, p < 0·0001), obsessive-compulsive disorder (CYBOCS-II, p = 0·0001), tics (YGTSS, p < 0·0001), attention-deficit hyperactivity disorder (Conner’s, p = 0·028), and overall quality of life (EQ-5D-Y, p = 0·011).
At baseline, the multi-omic approach revealed that leucocytes from patients with PANS had dysregulated epigenetic (chromatin structure, DNA methylation, histone modifications, transcription factors), ribosomal, mRNA processing, immune, and signalling pathways. These pathways were significantly modulated by NTI164 treatment.
NTI164 shows promise as a disease-modifying therapeutic for PANS.
Multi-omics reveal broad epigenetic and immune dysregulation in patients, which was modified by NTI164, presenting epigenetic machinery as a therapeutic target in PANS.”
“Cannabis sativa L. has long been used in medicine, and increasingly proposed as a treatment of psychiatric disorders and neurodevelopmental disorders (NDDs).”
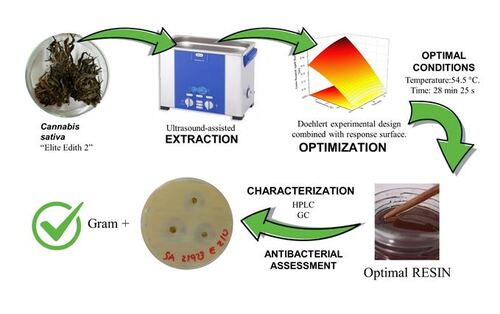
“Objective: To develop a green and efficient ultrasound-assisted extraction (UAE) process to obtain bioactive resins from Cannabis sativa with potential pharmaceutical applications, optimizing extraction parameters to maximize antioxidant capacity and total polyphenol content.
Significance: UAE using ethanol under mild temperature and time conditions as a green technique was applied to reduce solvent consumption, energy demand, and extraction time while preserving thermolabile bioactive compounds. Optimizing UAE enables the recovery of cannabinoid- and terpene-rich extracts that may serve as natural active pharmaceutical ingredients or functional excipients for drug development. This study integrate a Doehlert-based optimization of UAE with a functional evaluation of antioxidant efficiency and antimicrobial activity, providing a comprehensive framework for the development of cannabis-derived pharmaceutical ingredients.
Methods: A Doehlert experimental design combined with response surface methodology was employed to optimize temperature and extraction time. The optimized extract was characterized for its phytochemical composition. Antimicrobial activity was evaluated against Gram-positive and Gram-negative bacterial strains to assess potential therapeutic relevance.
Results: Under optimal conditions (54.5 °C, 28 min 25 s), the extract showed a total phenolic content of approximately 0.11 mg gallic acid/mg resin and an IC50 value of about 0.24 mg resin/mL extract, indicating enhanced antioxidant performance compared to non-optimized conditions. Also, showed selective bactericidal activity against Staphylococcus aureus ATCC 25923 and Staphylococcus epidermidis ATCC 12228, while Gram-negative strains remained resistant.
Conclusions: UAE extraction efficiently recovered antioxidant and selectively antimicrobial compounds from Cannabis sativa resins under mild, eco-friendly conditions, supporting their potential use as bioactive ingredients in pharmaceuticals.”