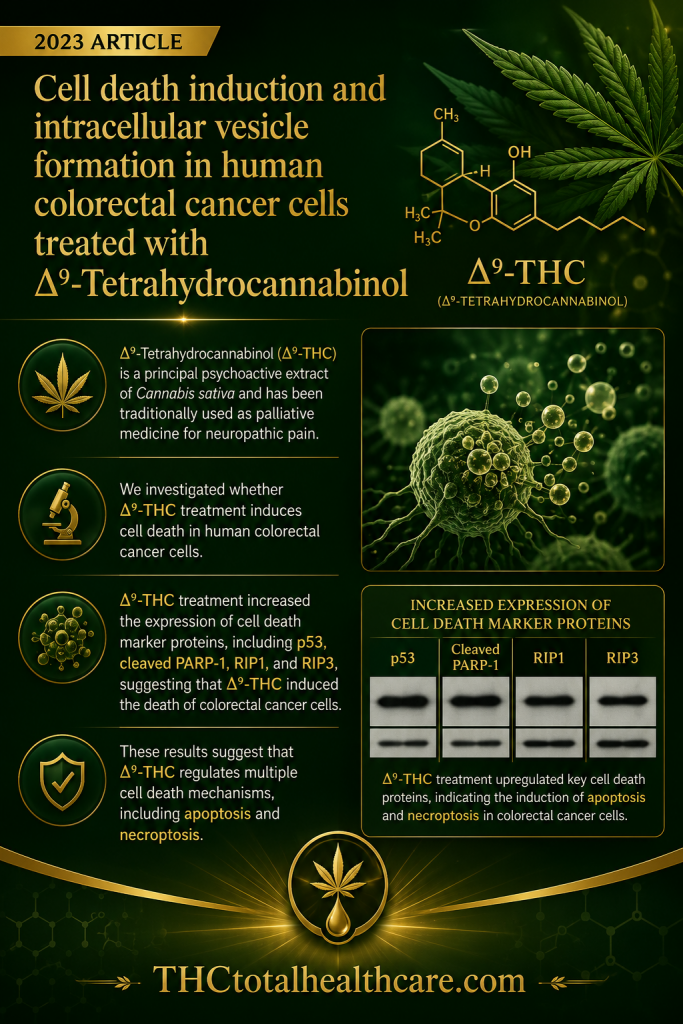
“Background: Δ9-Tetrahydrocannabinol (Δ9-THC) is a principal psychoactive extract of Cannabis sativa and has been traditionally used as palliative medicine for neuropathic pain. Cannabidiol (CBD), an extract of hemp species, has recently attracted increased attention as a cancer treatment, but Δ9-THC is also requiring explored pharmacological application.
Objective: This study evaluated the pharmacological effects of Δ9-THC in two human colorectal cancer cell lines. We investigated whether Δ9-THC treatment induces cell death in human colorectal cancer cells.
Methods: We performed an MTT assay to determine the pharmacological concentration of Δ9-THC. Annxein V and Western blot analysis confirmed that Δ9-THC induced apoptosis in colorectal cancer cells. Metabolic activity was evaluated using MitoTracker staining and ATP determination. We investigated vesicle formation by Δ9-THC treatment using GW9662, known as a PPARγ inhibitor.
Results: The MTT assay showed that treatment with 40 μM Δ9-THC and above inhibited the proliferation of colorectal cancer cells. Multiple intracytoplasmic vesicles were detected upon microscopic observation, and fluorescence-activated cell sorting analysis showed cell death via G1 arrest. Δ9-THC treatment increased the expression of cell death marker proteins, including p53, cleaved PARP-1, RIP1, and RIP3, suggesting that Δ9-THC induced the death of colorectal cancer cells. Δ9-THC treatment also reduced ATP production via changes in Bax and Bcl-2. Δ9-THC regulated intracytoplasmic vesicle formation by modulating the expression of PPARγ and clathrin, adding that antiproliferative activity of Δ9-THC was also affected.
Conclusion: In conclusion, Δ9-THC regulated two functional mechanisms, intracellular vesicle formation and cell death. These findings can help to determine how cannabinoids can be used most effectively to improve the efficacy of cancer treatment.”
https://pubmed.ncbi.nlm.nih.gov/37837516
“Cannabinoid extracts exhibit pharmacological effects by regulating the endocannabinoid system.”
“Δ9-THC treatment shows cell death and morphological changes in human colorectal cancer cells.”
“Therefore, these results suggest that Δ9-THC treatment induced cell death by inhibiting cell growth and inducing cellular morphological changes.”
https://link.springer.com/article/10.1007/s13258-023-01466-7