“The coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory distress syndrome coronavirus 2 (SARS-Cov-2), was identified for the first time in late 2019 in China, resulting in a global pandemic of massive impact. Despite a fast development and implementation of vaccination strategies, and the scouting of several pharmacological treatments, alternative effective treatments are still needed. In this regard, cannabinoids represent a promising approach because they have been proven to exhibit several immunomodulatory, anti-inflammatory, and antiviral properties in COVID-19 disease models and related pathological conditions. This mini-review aims at providing a practical brief overview of the potential applications of cannabinoids so far identified for the treatment and prevention of COVID-19, finally considering key aspects related to their technological and clinical implementation.”
“Overall, cannabinoids offer a great pharmacological potential in the management of COVID-19. It is to be hoped that the scientific evidence so far reported on cannabinoids effects along with the possibilities offered by drug delivery systems will entice the development of valuable therapies in this area.”
“The endocannabinoid system has been postulated to help restrict cancer progression and maintain osteoblastic function during bone metastasis. Herein, the effects of cannabinoid receptor (CB) type 1 and 2 activation on breast cancer cell and osteoblast interaction were investigated by using ACEA and GW405833 as CB1 and CB2 agonists, respectively. Our results showed that breast cancer cell (MDA-MB-231)-derived conditioned media markedly decreased osteoblast-like UMR-106 cell viability. In contrast, media from MDA-MB-231 cells pre-treated with GW405833 improved UMR-106 cell viability. MDA-MB-231 cells were apparently more susceptible to both CB agonists than UMR-106 cells. Thereafter, we sought to answer the question as to how CB agonists reduced MDA-MB-231 cell virulence. Present data showed that co-activation of CB1 and CB2 exerted cytotoxic effects on MDA-MB-231 cells by increasing apoptotic cell death through suppression of the NF-κB signaling pathway in an ROS-independent mechanism. ACEA or GW405833 alone or in combination also inhibited MDA-MB-231 cell migration. Thus, it can be concluded that the endocannabinoid system is able to provide protection during breast cancer bone metastasis by interfering cancer and bone cell interaction as well as by the direct suppression of cancer cell growth and migration.”
“In conclusions, we have demonstrated that the ECS—which was present in bone microenvironment—provided a protection against breast cancer bone metastasis and its negative consequence on bone cell survival. Specifically, CB agonists, especially CB2 agonist, was able to prevent breast cancer-induced osteoblast suppression. Each of the two CB agonists or a combination of both could reduce breast cancer cell survival and migration through the NF-κB-dependent pathway. “
“Rheumatoid arthritis (RA) is a painful chronic autoimmune disease affecting the joints. Its first-line therapy, Methotrexate (MTX), although effective in ameliorating the progress of the disease, induces hepatotoxicity over long-term usage. Thus, seeking natural compounds with fewer side effects could be an alternative therapeutic approach. This study aimed to investigate the anti-inflammatory, antiarthritic, and antioxidative effects of synthetic trans-Δ9-tetrahydrocannabinol (Δ9-THC) dissolved in sesame oil (Dronabinol) against MTX in adjuvant-induced arthritis (AIA) rat model. Daily oral administration of Δ9-THC/sesame oil, over a period of 21 days, was well tolerated in arthritic rats with no particular psychoactive side effects. It markedly attenuated the severity of clinical manifestations, recovered the histopathological changes in tibiotarsal joints, and repressed the splenomegaly in arthritic rats. Δ9-THC/sesame oil therapy showed similar effects to MTX in neutralizing the inflammatory process of AIA, through attenuating erythrocyte sedimentation rate (ESR) scores and proinflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin 1-beta (IL-1β), and interleukin-6 (IL-6) levels, to normal values. As opposed to MTX, this natural combination markedly protected the liver of arthritic rats and downregulated the induced oxidative stress by increasing the antioxidant defense system such as activities of catalase and superoxide dismutase (SOD) and levels of glutathione (GSH). These results suggest promising effects for the clinical use of Δ9-THC/sesame oil therapy in alleviating arthritic clinical signs as well as arthritis-induced liver injury.”
“Dronabinol (Δ9-THC in sesame oil) is usually used to treat nausea and vomiting caused by chemotherapy or weight loss and loss of appetite in AIDS patients, yet, to the best of our knowledge, this is the first study that proves the antiarthritic and antioxidative effects of this combination in an experimental model of RA with a hepatoprotective effect against arthritis-induced liver injury compared to commonly used antirheumatic drug (MTX).”
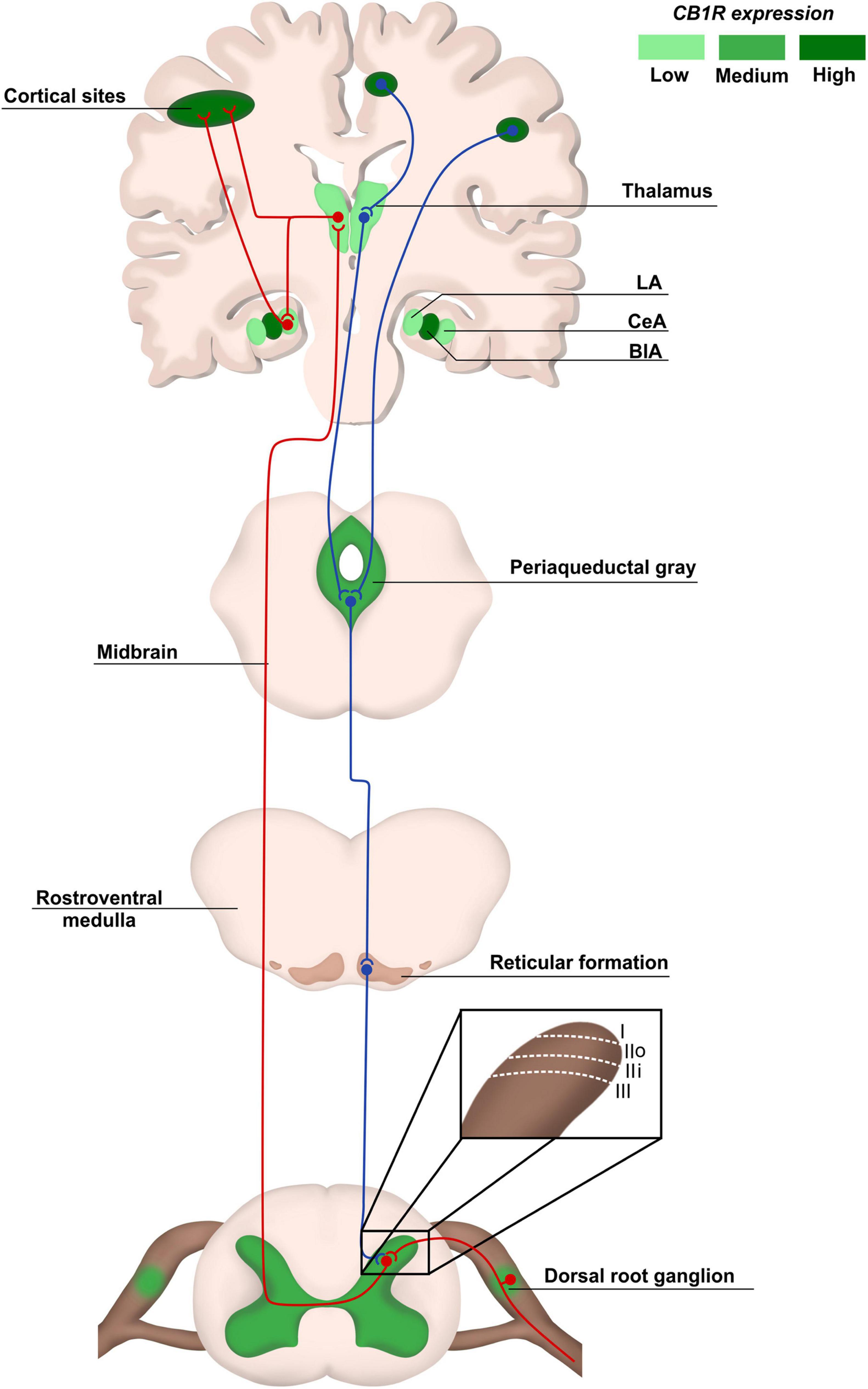
“Despite the importance of pain as a warning physiological system, chronic neuropathic pain is frequently caused by damage in the nervous system, followed by persistence over a long period, even in the absence of dangerous stimuli or after healing of injuries. Chronic neuropathic pain affects hundreds of millions of adults worldwide, creating a direct impact on quality of life. This pathology has been extensively characterized concerning its cellular and molecular mechanisms, and the endocannabinoid system (eCS) is widely recognized as pivotal in the development of chronic neuropathic pain. Scientific evidence has supported that phyto-, synthetic and endocannabinoids are efficient for pain management, while strong data arise from the therapeutic use of Cannabis-derived products. The use of medicinal Cannabis products is directed toward not only relieving symptoms of chronic pain, but also improving several aspects of patients’ welfare. Here, we review the involvement of eCS, along with other cellular and molecular elements, in chronic neuropathic pain pathology and how this system can be targeted for pain management.”
“The role of eCS as a pharmacological target and the advantages of using medicinal Cannabis sp. to treat pain is remarkable, as described in this review.”
“Background: Multiple therapeutic properties have been attributed to Cannabis sativa. However, further research is required to unveil the medicinal potential of Cannabis and the relationship between biological activity and chemical profile.
Objectives: The primary objective of this study was to characterize the chemical profile and antioxidant properties of three varieties of Cannabis sativa available in Uruguay during progressive stages of maturation.
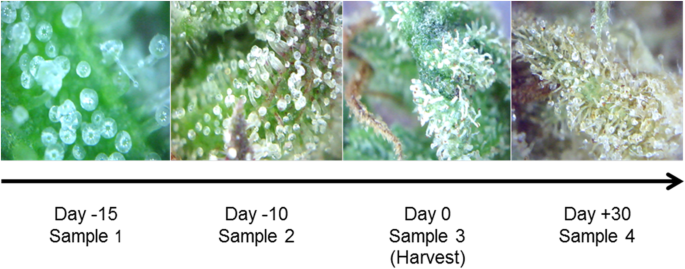
Methods: Fresh samples of female inflorescences from three stable Cannabis sativa phenotypes, collected at different time points during the end of the flowering period were analyzed. Chemical characterization of chloroform extracts was performed by 1H-NMR. The antioxidant properties of the cannabis sativa extracts, and pure cannabinoids, were measured in a Cu2+-induced LDL oxidation assay.
Results: The main cannabinoids in the youngest inflorescences were tetrahydrocannabinolic acid (THC-A, 242 ± 62 mg/g) and tetrahydrocannabinol (THC, 7.3 ± 6.5 mg/g). Cannabinoid levels increased more than twice in two of the mature samples. A third sample showed a lower and constant concentration of THC-A and THC (177 ± 25 and 1 ± 1, respectively). The THC-A/THC rich cannabis extracts increased the latency phase of LDL oxidation by a factor of 1.2-3.5 per μg, and slowed down the propagation phase of lipoperoxidation (IC50 1.7-4.6 μg/mL). Hemp, a cannabidiol (CBD, 198 mg/g) and cannabidiolic acid (CBD-A, 92 mg/g) rich variety, also prevented the formation of conjugated dienes during LDL oxidation. In fact, 1 μg of extract was able to stretch the latency phase 3.7 times and also to significantly reduce the steepness of the propagation phase (IC50 of 8 μg/mL). Synthetic THC lengthened the duration of the lag phase by a factor of 21 per μg, while for the propagation phase showed an IC50 ≤ 1 μg/mL. Conversely, THC-A was unable to improve any parameter. Meanwhile, the presence of 1 μg of pure CBD and CBD-A increased the initial latency phase 4.8 and 9.4 times, respectively, but did not have an effect on the propagation phase.
Conclusion: Cannabis whole extracts acted on both phases of lipid oxidation in copper challenged LDL. Those effects were just partially related with the content of cannabinoids and partially recapitulated by isolated pure cannabinoids. Our results support the potentially beneficial effects of cannabis sativa whole extracts on the initial phase of atherosclerosis.”
“Our findings support the beneficial effects of Cannabis sativa extracts on the initial phase of atherosclerosis. Since isolated cannabinoids were less effective preventing the oxidation of LDL, a synergistic effect between the diverse arrange of phytochemicals present in complex extracts is supported, reinforcing the entourage hypothesis and the use of whole medicinal cannabis extracts for therapeutic purposes.”
“Reduced brain glucose consumption arising from impaired glucose uptake and utilization has been linked to the pathogenesis and complications of neurodegenerative diseases. The ability of Cannabis sativa L. tetrahydrocannabinol (THC)-rich extracts to stimulate brain glucose uptake and utilization as well as its modulatory effect on gluconeogenesis, antioxidative, purinergic and cholinergic activities were investigated in isolated rats’ brains. C. sativa leaves were sequentially extracted to yield the hexane and dichloromethane extracts. The extracts were incubated at 37°C with freshly harvested brains in the presence of glucose for 2 h. The control consisted of incubation without the extracts, while brains without the extracts and glucose served as the normal control. Metformin was used as the standard drug. C. sativa extracts caused a significant (p < 0.05) increase in brain glucose uptake, with concomitant elevation of glutathione level, superoxide dismutase, catalase, and ecto-nucleoside triphosphate diphosphohydrolase activities compared to the controls. Incubation with C. sativa extracts also led to depletion in malondialdehyde and nitric oxide levels, acetylcholinesterase, butyrylcholinesterase, glucose 6-phosphatase and fructose-1,6-biphosphatase activities. GC-MS analysis of the extracts revealed the presence of THC. In silico analysis predicted THC to be permeable across the blood-brain-barrier. THC was also predicted to have an oral LD50 and toxicity class values of 482 mg/kg and 4 respectively. These results indicate that C. sativa improves glucose consumption with concomitant suppression of oxidative stress and cholinergic dysfunction, and modulation of purinergic and gluconeogenic activities in brain tissues.”
“As portrayed by these results, C. sativa improves glucose consumption with concomitant suppression of oxidative stress and cholinergic dysfunction, and modulation of purinergic and gluconeogenic activities in brain tissues. Further studies are recommended to decipher the molecular mechanisms that may be involved in these neuroprotective activities in in vivo studies.”
“Cannabis sativa L. is a crop utilized globally for recreational, therapeutic, and religious purposes. Although considered as an illicit drug in most countries, C. sativa until recently started gaining attention for its medicinal application. This study sought to investigate the hepatoprotective effect of C. sativa on iron-mediated oxidative hepatic injury. Hepatic injury was induced ex vivo by incubating hepatic tissues with Fe2+, which led to depleted levels of reduced glutathione, superoxide dismutase, catalase and ENTPDase activities, triglyceride, and high-density lipoprotein-cholesterol (HDL-C). Induction of hepatic injury also caused significant elevation of malondialdehyde, nitric oxide, cholesterol, and low-density lipoprotein-cholesterol (LDL-C) levels while concomitantly elevating the activities of ATPase, glycogen phosphorylase, glucose-6-phosphatase, fructose-1,6-bisphosphatase, amylase, and lipase. Treatment with the hexane, dichloromethane (DCM), and ethanol extracts of C. sativa leaves significantly (p < 0.05) reversed these levels and activities to almost near normal. However, there was no significant effect on the HDL-C level. The extracts also improved the utilization of glucose in Chang liver cells. High-performance liquid chromatography (HPLC) analysis showed the presence of phenolics in all extracts, with the ethanol extract having the highest constituents. Cannabidiol (CBD) was identified in all the extracts, while Δ-9-tetrahydrocannabinol (Δ-9-THC) was identified in the hexane and DCM extracts only. Molecular docking studies revealed strong interactions between CBD and Δ-9-THC with the β2 adrenergic receptor of the adrenergic system. The results demonstrate the potential of C. sativa to protect against oxidative-mediated hepatic injury by stalling oxidative stress, gluconeogenesis, and hepatic lipid accumulation while modulating cholinergic and purinergic activities. These activities may be associated with the synergistic effect of the compounds identified and possible interactions with the adrenergic system.”
“The data obtained in this study indicate the ability of C. sativa to protect against oxidative-mediated hepatic injury by stalling oxidative stress, gluconeogenesis, and hepatic lipid accumulation while modulating cholinergic and purinergic activities. These activities may be associated with the synergistic effect of the identified phenolics, CBD, and Δ-9-THC and possible interactions with the adrenergic system.”
“Background: A small body of evidence suggests medical cannabis may facilitate wound healing, but the exact mechanism of this effect is unclear.
Purpose: This case report describes a patient with a pressure injury (PI) who received cannabis oil treatment for pain management and sleep improvement.
Methods: A 37-year-old woman with multiminicore disease, scoliosis, short-chain acyl-CoA dehydrogenase deficiency, and epilepsy presented to the Neurology Centre of Toronto with chronic pain and sleep disturbance, including difficulty initiating and maintaining sleep. She also had a 5-year history of a PI between her right iliac crest and right rib cage that had progressively worsened. The patient received a medical cannabis oil protocol that used a combination of cannabidiol and tetrahydrocannabinol.
Results: Cannabis oil was effective in treating pain and sleep difficulties. Unexpectedly, during the first 2 weeks of treatment, the PI started to heal and was almost completely closed at the 2-month follow-up.
Conclusion: Although it is unknown if the observed healing of this refractory PI was indirectly or directly related to the cannabidiol and tetrahydrocannabinol treatment, the potential relationships among pain, sleep disturbance, cannabis treatment, and healing should be explored.”
“This case report provides an account of a patient who began using orally administered medical cannabis oil for sleep disturbances and pain management and subsequently experienced rapid healing of a chronic PI.”
“Background: Despite the absence of rigorous prospective studies, there has been an increase in the use of cannabis-based medicinal products. During the study period, the use of medical cannabis in Israel was tightly regulated by national policy. Through a prospective study of approximately 10,000 patients, we aimed to characterize the medical cannabis patient population as well as to identify treatment adherence, safety, and effectiveness.
Methods and findings: In this study of prescribed medical cannabis patients, adherence, safety, and effectiveness were assessed at 6 months. Treatment adherence was assessed by the proportion of patients purchasing the medication out of the total number of patients (excluding deceased cases and patients transferred to another cannabis clinic). Safety was assessed by the frequency of the side-effects, while effectiveness was defined as at least moderate improvement in the patient condition without treatment cessation or serious side-effects. The most frequent primary indications requiring therapy were cancer (49.1%), followed by non-specific pain (29.3%). The average age was 54.6 ± 20.9 years, 51.1% males; 30.2% of the patients reported prior experience with cannabis. During the study follow-up, 1,938 patients died (19.4%) and 1,735 stopped treatment (17.3%). Common side-effects, reported by 1,675 patients (34.2%), were: dizziness (8.2%), dry mouth (6.7%), increased appetite (4.7%), sleepiness (4.4%), and psychoactive effect (4.3%). Overall, 70.6% patients had treatment success at 6 months. Multivariable logistic regression analysis revealed that the following factors were associated with treatment success: cigarette smoking, prior experience with cannabis, active driving, working, and a young age. The main limitation of this study was the lack of data on safety and effectiveness of the treatment for patients who refused to undergo medical assessment even at baseline or died within the first 6 months.
Conclusions: We observed that supervised medical-cannabis treatment is associated with high adherence, improvement in quality of life, and a decrease in pain level with a low incidence of serious adverse events.”
“This is a large study describing certain characteristics of medical cannabis users in a tightly regulated environment. The treatment appears to be safe and efficacious.”
“Objectives: Assessing the effectiveness and tolerability of medical cannabis (MC) treatment on Gilles de la Tourette syndrome (GTS) patients.
Methods: We report on an open-label, prospective study on the effect of MC on adult GTS patients. MC mode of use was decided by the treating neurologist and the patient. Δ9-Tetrahydrocannabinol (Δ9-THC) and cannabidiol (CBD) content within MC product and monthly dose were titrated during the study. Following treatment initiation, patients were assessed after 4 and 12 weeks for efficacy, tolerability, and side effects.
Results: Eighteen patients entered the study. Baseline Yale Global Tic Severity Scale- (YGTSS) Total (range 0-100) was 60.3 ± 17.1. Three patients did not reach the end of follow-up period. The most common mode of administration was smoking (80%). Following twelve weeks of treatment, a significant 38% average reduction (p = 0.002) of YGTSS-Total and a 20% reduction (p = 0.043) of Premonitory Urge for Tic Scale (PUTS) were observed. Common side effects were dry mouth (66.7%), fatigue (53.3%), and dizziness (46.7%). Three patients suffered from psychiatric side effects including worsening of obsessive compulsive disorder (stopped treatment), panic attack, and anxiety (resolved with treatment modification). Six patients (40%) reported cognitive side effects regarding time perception, visuospatial disorientation, confusion, slow processing speed, and attention.
Conclusions: MC treatment demonstrates good efficacy and tolerability in adult GTS patients. Predilection for smoking rather than using oil drops requires further comparative studies to evaluate the efficacy of each. Cognitive and psychiatric side effects have to be monitored and addressed.”
“Our results are in line with a number of other studies suggesting that MC is effective and well tolerated in adults with GTS. From our data, it is suggested that MC might be a treatment option for resistant TS patients, and MC has a significant effect on tics, premonitory urges, and patients’ overall quality of life. In our sample, patients favored THC-rich cannabis strands and smoking/inhaling MC over sublingual oil.”