“Chronic adolescent exposure to Δ-9-Tetrahydrocannabinol (THC) is linked to elevated neuropsychiatric risk and induces neuronal, molecular and behavioural abnormalities resembling neuropsychiatric endophenotypes. Previous evidence has revealed that the mesocorticolimbic circuitry, including the prefrontal cortex (PFC) and mesolimbic dopamine (DA) pathway are particularly susceptible to THC-induced pathological alterations, including dysregulation of DAergic activity states, loss of PFC GABAergic inhibitory control and affective and cognitive abnormalities. There are currently limited pharmacological intervention strategies capable of preventing THC-induced neuropathological adaptations.
“Chronic adolescent exposure to Δ-9-Tetrahydrocannabinol (THC) is linked to elevated neuropsychiatric risk and induces neuronal, molecular and behavioural abnormalities resembling neuropsychiatric endophenotypes. Previous evidence has revealed that the mesocorticolimbic circuitry, including the prefrontal cortex (PFC) and mesolimbic dopamine (DA) pathway are particularly susceptible to THC-induced pathological alterations, including dysregulation of DAergic activity states, loss of PFC GABAergic inhibitory control and affective and cognitive abnormalities. There are currently limited pharmacological intervention strategies capable of preventing THC-induced neuropathological adaptations.
L-theanine is an amino acid analogue of L-glutamate and L-glutamine derived from various plant sources, including green tea leaves. L-theanine has previously been shown to modulate levels of GABA, DA and glutamate in various neural regions and to possess neuroprotective properties.
Using a pre-clinical model of adolescent THC exposure in male rats, we report that L-theanine pre-treatment prior to adolescent THC exposure is capable of preventing long-term, THC-induced dysregulation of both PFC and VTA DAergic activity states, a neuroprotective effect which persists into adulthood. In addition, pre-treatment with L-theanine blocked THC-induced downregulation of local GSK-3 and Akt signaling pathways directly in the PFC, two biomarkers previously associated with cannabis-related psychiatric risk and sub-cortical DAergic dysregulation.
Finally, L-theanine powerfully blocked the development of both affective and cognitive abnormalities commonly associated with adolescent THC exposure, further demonstrating functional and long-term neuroprotective effects of L-theanine in the mesocorticolimbic system.
SIGNIFICANCE STATEMENT With the increasing trend of cannabis legalization and consumption during adolescence, it is essential to expand knowledge on the potential effects of adolescent cannabis exposure on brain development and identify potential pharmacological strategies to minimize THC-induced neuropathology. Previous evidence demonstrates that adolescent THC exposure induces long-lasting affective and cognitive abnormalities, mesocorticolimbic dysregulation and schizophrenia-like molecular biomarkers that persist into adulthood.
We demonstrate for the first time that L-theanine, an amino acid analogue of L-glutamate and L-glutamine, is capable of preventing long-term THC side-effects. L-theanine prevented development of THC-induced behavioral aberrations, blocked cortical downregulation of local GSK-3 and Akt signaling pathways and normalized dysregulation of both PFC and VTA DAergic activity, demonstrating powerful and functional neuroprotective effects against THC-induced developmental neuropathology.”
https://pubmed.ncbi.nlm.nih.gov/33268546/
https://www.jneurosci.org/content/early/2020/11/24/JNEUROSCI.1050-20.2020

 “Plant-based therapies date back centuries. Cannabis sativa is one such plant that was used medicinally up until the early part of the 20th century.
“Plant-based therapies date back centuries. Cannabis sativa is one such plant that was used medicinally up until the early part of the 20th century.
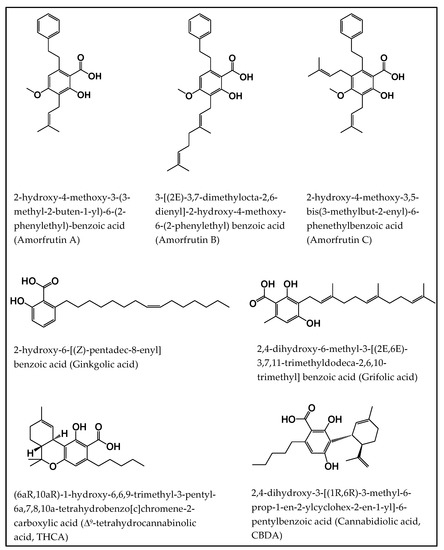
 “Cannabis sativa L. is an aromatic annual herb belonging to the family Cannabaceae and it is widely distributed worldwide. Cultivation, selling, and consumption of cannabis and cannabis related products, regardless of its use, was prohibited in Lebanon until April 22, 2020. Nevertheless, cannabis oil has been traditionally used unlawfully for many years in Lebanon to treat diseases such as arthritis, diabetes, cancer and few neurological disorders.
“Cannabis sativa L. is an aromatic annual herb belonging to the family Cannabaceae and it is widely distributed worldwide. Cultivation, selling, and consumption of cannabis and cannabis related products, regardless of its use, was prohibited in Lebanon until April 22, 2020. Nevertheless, cannabis oil has been traditionally used unlawfully for many years in Lebanon to treat diseases such as arthritis, diabetes, cancer and few neurological disorders.
 “Stem cell therapy promotes tissue regeneration and wound healing. Efforts have been made to prime stem cells to enhance their regenerative abilities.
“Stem cell therapy promotes tissue regeneration and wound healing. Efforts have been made to prime stem cells to enhance their regenerative abilities. “A significant number of cannabinoids are known to have analgesic and anti-inflammatory properties in various diseases. Due to their presynaptic/terminal location, cannabinoid receptors can inhibit synaptic transmission and have the potential to regulate neurogenic inflammation. Neurogenic inflammation occurs when a noxious signal is detected in the periphery initiating an antidromic axon reflex in the same sensory neurone leading to depolarization of the afferent terminal. Neuropeptides are subsequently released and contribute to vasodilation, plasma extravasation and modulation of immune cells. Endocannabinoids, synthetic cannabinoids and phytocannabinoids can reduce neuroinflammation by inhibiting afferent firing and inflammatory neuropeptide release. Thus, in addition to a direct effect on vascular smooth muscle and inflammatory cells, cannabinoids can reduce inflammation by silencing small diameter neurones. This review examines the neuropharmacological processes involved in regulating antidromic depolarization of afferent nerve terminals by cannabinoids and the control of neurogenic inflammation in different diseases.”
“A significant number of cannabinoids are known to have analgesic and anti-inflammatory properties in various diseases. Due to their presynaptic/terminal location, cannabinoid receptors can inhibit synaptic transmission and have the potential to regulate neurogenic inflammation. Neurogenic inflammation occurs when a noxious signal is detected in the periphery initiating an antidromic axon reflex in the same sensory neurone leading to depolarization of the afferent terminal. Neuropeptides are subsequently released and contribute to vasodilation, plasma extravasation and modulation of immune cells. Endocannabinoids, synthetic cannabinoids and phytocannabinoids can reduce neuroinflammation by inhibiting afferent firing and inflammatory neuropeptide release. Thus, in addition to a direct effect on vascular smooth muscle and inflammatory cells, cannabinoids can reduce inflammation by silencing small diameter neurones. This review examines the neuropharmacological processes involved in regulating antidromic depolarization of afferent nerve terminals by cannabinoids and the control of neurogenic inflammation in different diseases.” “Effective treatment choices to the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) are limited because of the absence of effective target-based therapeutics. The main object of the current research was to estimate the antiviral activity of cannabinoids (CBDs) against the human coronavirus SARS-CoV-2.
“Effective treatment choices to the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) are limited because of the absence of effective target-based therapeutics. The main object of the current research was to estimate the antiviral activity of cannabinoids (CBDs) against the human coronavirus SARS-CoV-2.
 “Cannabis sativa is a well-known plant which has been of benefit since ancient times in several medicinal systems, including Chinese, Indian, Greek and Egyptian ones.
“Cannabis sativa is a well-known plant which has been of benefit since ancient times in several medicinal systems, including Chinese, Indian, Greek and Egyptian ones.