“Breast cancer is the leading cause of cancer-related death in women worldwide. In the last years, cannabinoids have gained attention in the clinical setting and clinical trials with cannabinoid-based preparations are underway. However, contradictory anti-tumour properties have also been reported. Thus, the elucidation of the molecular mechanisms behind their anti-tumour efficacy is crucial to better understand its therapeutic potential.
“Breast cancer is the leading cause of cancer-related death in women worldwide. In the last years, cannabinoids have gained attention in the clinical setting and clinical trials with cannabinoid-based preparations are underway. However, contradictory anti-tumour properties have also been reported. Thus, the elucidation of the molecular mechanisms behind their anti-tumour efficacy is crucial to better understand its therapeutic potential.
Considering this, our work aims to clarify the molecular mechanisms underlying the anti-cancer properties of the endocannabinoid anandamide (AEA) and of the phytocannabinoids, cannabidiol (CBD) and Δ9-tetrahydrocannabinol (THC), in estrogen receptor-positive (ER+) breast cancer cells that overexpress aromatase (MCF-7aro). Their in vitro effects on cell proliferation, cell death and activity/expression of aromatase, ERα, ERβ and AR were investigated.
Our results demonstrated that cannabinoids disrupted MCF-7aro cell cycle progression. Unlike AEA and THC that induced apoptosis, CBD triggered autophagy to promote apoptotic cell death. Interestingly, all cannabinoids reduced aromatase and ERα expression levels in cells. On the other hand, AEA and CBD not only exhibited high anti-aromatase activity but also induced up-regulation of ERβ. Therefore, all cannabinoids, albeit by different actions, target aromatase and ERs, impairing, in that way, the growth of ER+ breast cancer cells, which is dependent on estrogen signalling.
As aromatase and ERs are key targets for ER+ breast cancer treatment, cannabinoids can be considered as potential and attractive therapeutic compounds for this type of cancer, being CBD the most promising one. Thus, from an in vitro perspective, this work may contribute to the growing mass of evidence of cannabinoids and cannabinoids-based medicines as potential anti-cancer drugs.”
https://pubmed.ncbi.nlm.nih.gov/33722705/
“AEA and THC induce apoptosis in ER+ breast cancer cells, while CBD trigger autophagy to promote apoptosis. AEA, THC and CBD impair growth of ER+ breast cancer cells, by disrupting cycle progression. AEA, THC and CBD affect aromatase and ERα expression levels in ER+ breast cancer cells. AEA and CBD strongly inhibited aromatase activity and up-regulated ERβ levels. Cannabinoids are considered potential therapeutic compounds for ER+ breast cancer, being CBD the most promising one.”
https://www.sciencedirect.com/science/article/abs/pii/S0960076021000698?via%3Dihub
 “The rapid spread of COVID-19 underscores the need for new treatments.
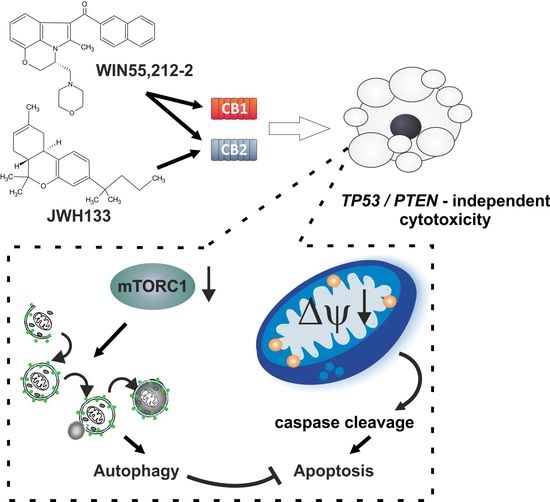
“The rapid spread of COVID-19 underscores the need for new treatments. “Cannabidiol (CBD) has been shown to slow cancer cell growth and is toxic to human glioblastoma cell lines. Thus, CBD could be an effective therapeutic for glioblastoma.
“Cannabidiol (CBD) has been shown to slow cancer cell growth and is toxic to human glioblastoma cell lines. Thus, CBD could be an effective therapeutic for glioblastoma.
 “Background: Breast Cancer (BC), a common death-causing disease and the deadliest cancer next to lung cancer, is characterized by an abnormal growth of cells in the tissues of the breast. BC chemotherapy is marked by targeting the activities of some receptors such as Estrogen Receptor alpha (ER-α). At present, one of the most commonly used and approved marketed therapeutic drug for BC is tamoxifen. Despite the short term success of tamoxifen usage, its long time treatment has been associated with significant side effects. Therefore, there is a pressing need for the development of novel anti-estrogens for the prevention and treatment of BC.
“Background: Breast Cancer (BC), a common death-causing disease and the deadliest cancer next to lung cancer, is characterized by an abnormal growth of cells in the tissues of the breast. BC chemotherapy is marked by targeting the activities of some receptors such as Estrogen Receptor alpha (ER-α). At present, one of the most commonly used and approved marketed therapeutic drug for BC is tamoxifen. Despite the short term success of tamoxifen usage, its long time treatment has been associated with significant side effects. Therefore, there is a pressing need for the development of novel anti-estrogens for the prevention and treatment of BC.


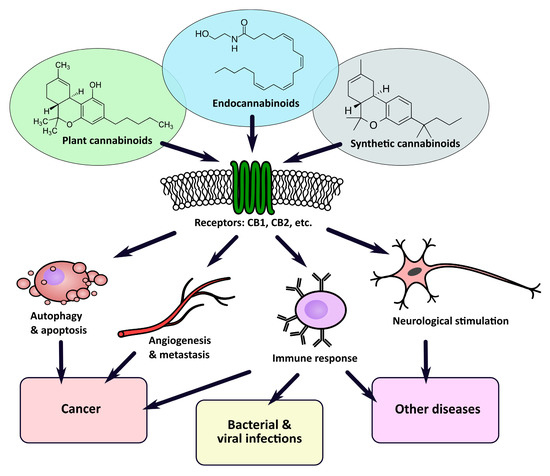
 “Derivatives of the plant Cannabis sativa have been used for centuries for both medical and recreational purposes, as well as industrial. The first proof of its medicinal use comes from ancient China, although there is evidence of its earlier utilization in Europe and Asia. In the 19th century, European practitioners started to employ cannabis extracts to treat tetanus, convulsions, and mental diseases and, in 1851, cannabis made its appearance in the Pharmacopoeia of the United States as an analgesic, hypnotic and anticonvulsant. It was only in 1937 that the Marijuana Tax Act prohibited the use of this drug in the USA. The general term Cannabis is commonly used by the scientific and scholar community to indicate derivatives of the plant Cannabis sativa. The word cannabinoid is a term describing chemical compounds that are either derivate of Cannabis (phytocannabinoids) or artificial analogues (synthetic) or are produced endogenously by the body (endocannabinoids). A more casual term “marijuana” or “weed”, a compound derived from dried Cannabis flower tops and leaves, has progressively superseded the term cannabis when referred to its recreational use. The 2018 World health organisation (WHO) data suggest that nearly 2.5% of the global population (147 million) uses marijuana and some countries, such as Canada and Uruguay, have already legalised it. Due to its controversial history, the medicinal use of cannabinoids has always been a centre of debate. The isolation and characterisation of Δ9 tetrahydrocannabinol (THC), the major psychoactive component of cannabis and the detection of two human cannabinoid receptor (CBRs) molecules renewed interest in the medical use of cannabinoids, boosting research and commercial heed in this sector. Some cannabinoid-based drugs have been approved as medications, mainly as antiemetic, antianorexic, anti-seizure remedies and in cancer and multiple sclerosis patients’ palliative care. Nevertheless, due to the stigma commonly associated with these compounds, cannabinoids’ potential in the treatment of conditions such as cancer is still largely unknown and therefore underestimated.”
“Derivatives of the plant Cannabis sativa have been used for centuries for both medical and recreational purposes, as well as industrial. The first proof of its medicinal use comes from ancient China, although there is evidence of its earlier utilization in Europe and Asia. In the 19th century, European practitioners started to employ cannabis extracts to treat tetanus, convulsions, and mental diseases and, in 1851, cannabis made its appearance in the Pharmacopoeia of the United States as an analgesic, hypnotic and anticonvulsant. It was only in 1937 that the Marijuana Tax Act prohibited the use of this drug in the USA. The general term Cannabis is commonly used by the scientific and scholar community to indicate derivatives of the plant Cannabis sativa. The word cannabinoid is a term describing chemical compounds that are either derivate of Cannabis (phytocannabinoids) or artificial analogues (synthetic) or are produced endogenously by the body (endocannabinoids). A more casual term “marijuana” or “weed”, a compound derived from dried Cannabis flower tops and leaves, has progressively superseded the term cannabis when referred to its recreational use. The 2018 World health organisation (WHO) data suggest that nearly 2.5% of the global population (147 million) uses marijuana and some countries, such as Canada and Uruguay, have already legalised it. Due to its controversial history, the medicinal use of cannabinoids has always been a centre of debate. The isolation and characterisation of Δ9 tetrahydrocannabinol (THC), the major psychoactive component of cannabis and the detection of two human cannabinoid receptor (CBRs) molecules renewed interest in the medical use of cannabinoids, boosting research and commercial heed in this sector. Some cannabinoid-based drugs have been approved as medications, mainly as antiemetic, antianorexic, anti-seizure remedies and in cancer and multiple sclerosis patients’ palliative care. Nevertheless, due to the stigma commonly associated with these compounds, cannabinoids’ potential in the treatment of conditions such as cancer is still largely unknown and therefore underestimated.”